
Diagnosing Outbound Pipeline Problems
Fourteen years on, we can still learn a thing or two from Dr. House.

The early 2000’s TV show House follows Hugh Laurie’s misanthropic Dr. House and his team of diagnosticians at a teaching hospital in New Jersey. It’s essentially a mystery-of-the-week show with a very predictable formula:
A sympathetic patient shows up with a super-weird disease.
House and team review symptoms, come up with ideas, and try a bunch of stuff to try to find the cause.
House—a brilliant, often drug-addicted, but lovable, jerk—insults a bunch of people, nearly kills the patient a couple of times but ultimately leads his team to a cure by the end of the 3rd act.
I was reminded of the show last week because Hugh Laurie’s response to a similar critique on X went viral:
We actually tried a couple episodes where House […] gets it right the first time, but they were only 6 minutes long. NBC wasn’t happy. Then we tried some where House never gets it right and the patient dies. The audience wasn’t happy.
Fair enough. The reason there’s dramatic tension in the formula is that there’s a very obvious problem (“a boy has mysterious bleeding and is seeing aliens”) but a very non-obvious solution (“he absorbed his twin in the womb and it’s trying to take over”)1. Solving that mystery—before time runs out for the patient—is what makes it compelling.
What, you might ask, does a broadcast dramedy that went off the air in 2012 have to do with GTM in 2026? Well, outbound teams find themselves playing out the same formulaic plot. A mysterious downward pipeline trend appears, the team furiously tries things, and (hopefully) the numbers improve. Then they do it all again next week, next month, next quarter.
Maybe we can learn a thing or two from Dr House.
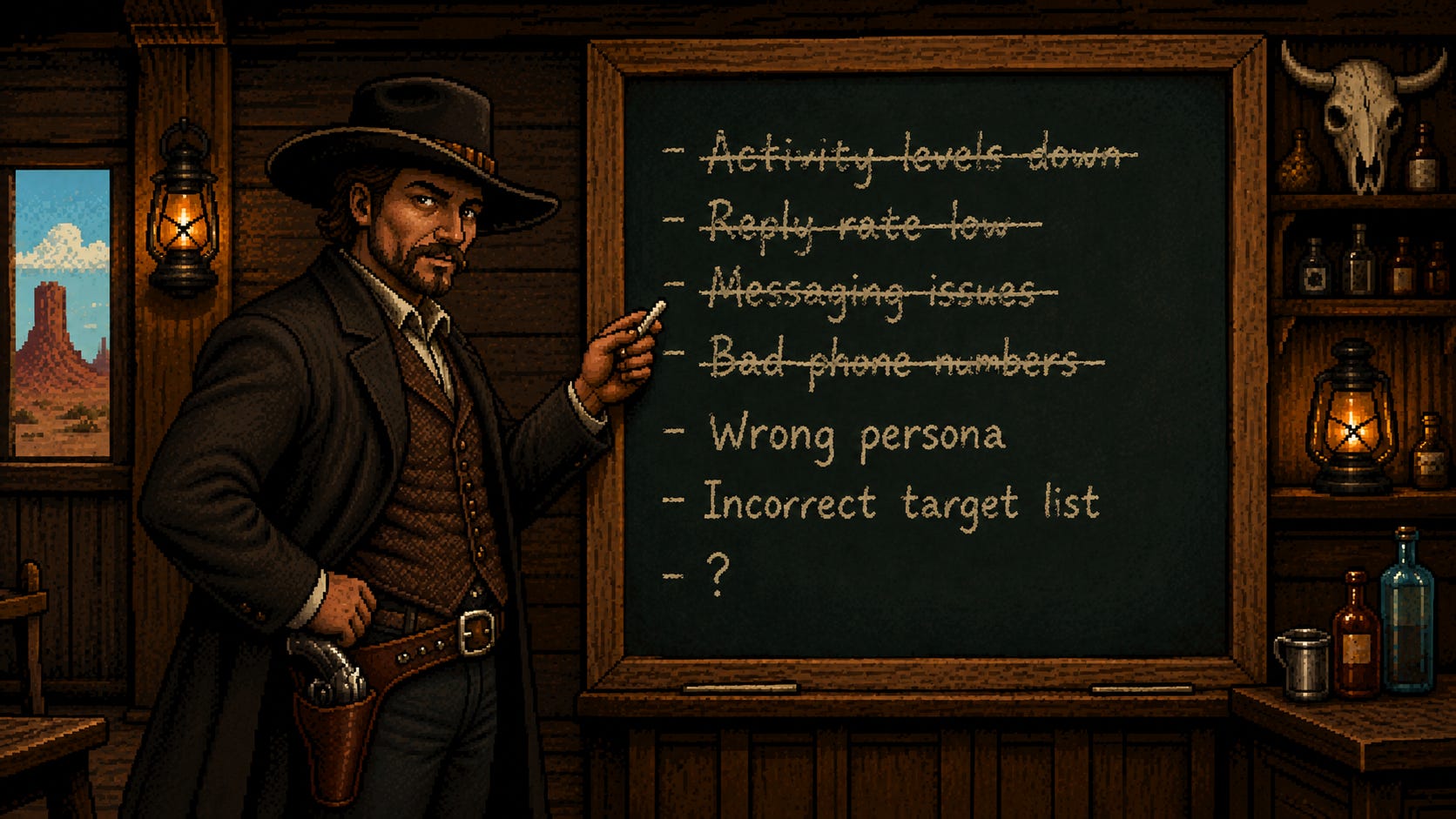
Act 1: A patient presents pipeline problems
I met with my friend Dave Breshears on Tuesday. Few people have thought more deeply about the process of outbound and diagnosed more outbound problems across more teams than Dave.2 While he’s not a jerk, he can sometimes be a bit cantankerous. He’s as close as you’ll get to the Dr. House of outbound.
Now I’ve written a thing or two on outbound myself. So in an effort to impress him, I shared a visual outline for a framework I’ve used to diagnose outbound issues. It sparked a conversation that led me to write this post.
You can see the diagram below:
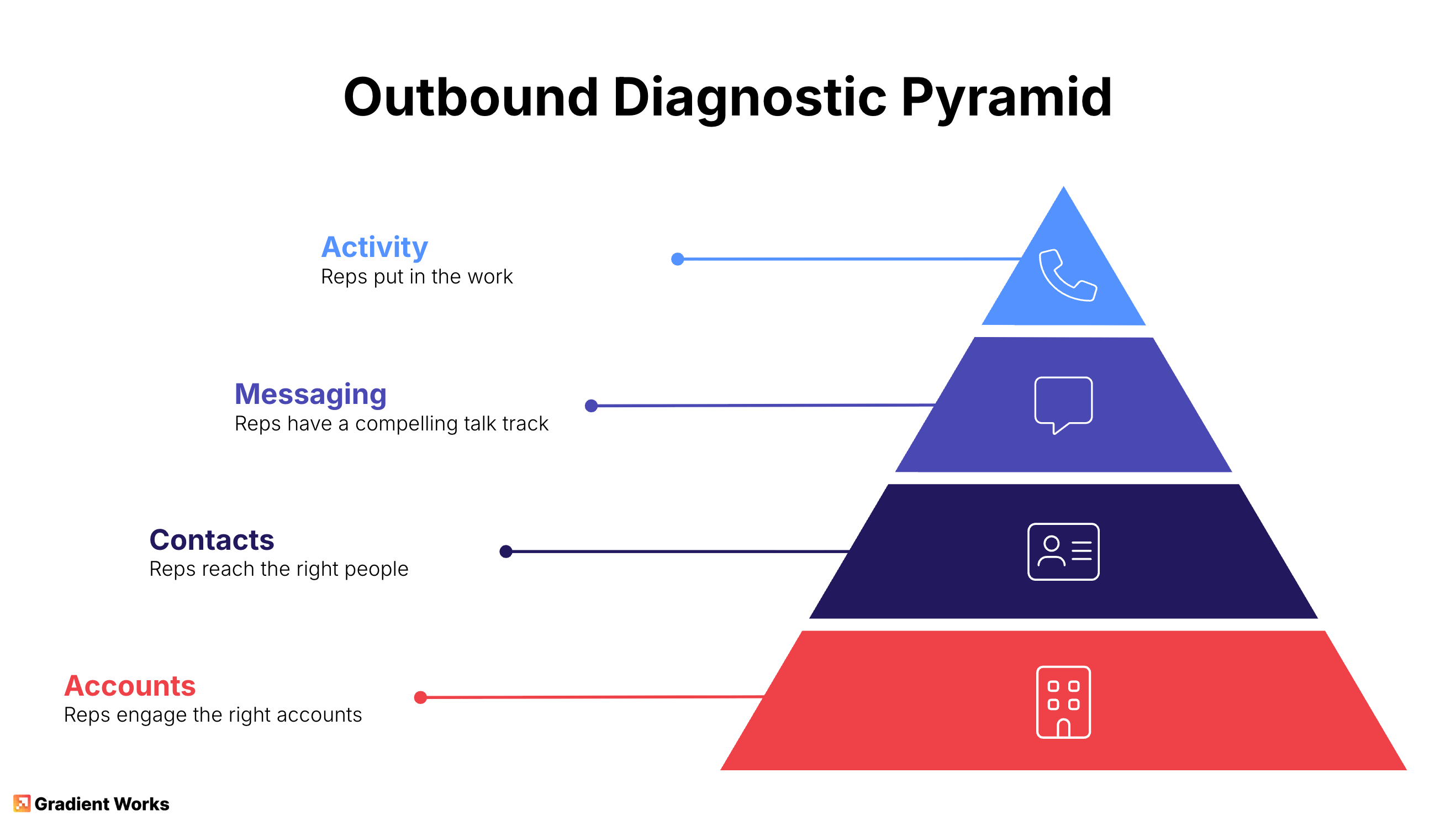
It’s a pyramid because each layer builds on the other. Accounts form the foundation. If I target the wrong accounts, nothing else matters, including the contacts I’m reaching out to. The world’s best messaging doesn’t matter if it doesn’t apply to the people hearing it. And finally, my reps can be nailing every activity target but that doesn’t matter if the accounts are bad, the personas are wrong, or the messaging doesn’t resonate.
The interesting thing is that it’s easier and faster to focus on problems at the top of the pyramid than it is to address the ones at the bottom. The farther down you go, the more teams need to get involved and the more work you need to do to firm up the foundation.
Guess where most sales leaders start when there’s a problem? The tippy-top.
When pipeline’s down, sales leaders focus on activity because it’s easy and obvious. It’s right there on a dashboard because even the world’s worst dashboards can count rep tasks. If activity isn’t where it needs to be, well, they apply the time honored solution to any sales problem: “motivate” the reps to do more.3 That may help, but only if that’s actually the root cause and not a symptom of a problem at a lower level.
That became the conversation Dave and I had. We agreed on the basic shape of the pyramid, but the devil’s very much in the details. How do you actually diagnose where the real problem lies? Which brings us back to House.
Act 2: Differential diagnosis
House plots can be outlandish, but Dr. House and his team use a real medical concept to try to solve their mysteries: differential diagnosis. The idea is to list all possible diseases associated with a set of symptoms and then rule out possible causes by finding things that aren’t consistent with a particular disease. Keep doing that and whatever’s left must be the answer.
This is an incredibly useful approach to solving a messy problem where multiple symptoms are present—a lot like any kind of outbound pipeline gap. Let’s see how we can apply it here.
The first thing most folks want to do is point to a single metric as the smoking gun that identifies where the real problem lies. It’s not that simple because most metrics an outbound team tracks can’t be isolated to a single layer. This means that, on their own, they’re not super useful for differential diagnosis.
Consider something basic like reply rate. This seems pretty firmly tied to the messaging layer—better messaging means more replies. However, a low reply rate could mean you’re sending to the wrong persona or that the accounts you’re targeting don’t have the problem your messaging highlights.
In fact, there are only a few metrics I can think of that are truly embedded in a single layer where underperformance might explicitly implicate that layer. And those are limited to just the activity and contact layers.
Activity layer - rep inputs like total activities, contacts sequenced, accounts engaged, sequences completed.
Contact layer - connect rate is a bit of a special case given that it’s a function of accurate contact phone numbers and dialing infrastructure.
It’s important to realize that even if these numbers aren’t great, it’s not clear that fixing them will actually help. In House, they’ll usually find something that’s clearly not right, treat it and then find the patient doesn’t get any better.
Other output or quality metrics—quota attainment, opportunity creation rate, reply rate, meetings held, sales acceptance rate, etc—aren’t directly tied to a layer at all so they don’t provide any clarity on root cause.
Ok, so the things we can clearly see are wrong may or may not help. The other things just tell us something’s wrong (which we already knew!) but not what to fix. How can we start to eliminate problems?
This is where you start looking at cohorts and controls to start ruling things out.
Let’s say you want to know if the activity layer is really the problem. Group your reps into cohorts based on how deeply they engage their accounts. Measure the opportunity output and the opportunity creation rates for each cohort. If the cohort with more engagement yields more opportunities without a decline in opportunity creation rate, then bringing the other cohorts up to the same level will actually make a difference. However, this only works if you control for messaging, contacts and accounts—ensuring they’re broadly the same across cohorts. That’s the only way you can rule those out as potential issues.
You can apply this concept to every other layer. Create cohorts of contacts by segmenting on seniority or function. Control for the amount of touches, messaging and accounts. You can do the same thing at the account layer by creating cohorts based on different firmographic cuts. Look for differences in key metrics.
A few iterations of this and you’ll begin to see a differential diagnosis take shape. For example, if reply rates are uniformly terrible across all contact cohorts and at all engagement levels, you likely have a messaging problem. If 3 cohorts respond well but a 4th doesn’t, you can probably rule out messaging as the root cause.
One word of warning: don’t slice too thin. A cohort with just a few members isn’t going to tell you much of anything. Just because the one zoo you reached out to took a meeting doesn’t mean that you need to change your entire outbound strategy to target zoos.
Finally, you don’t have to do all this diagnosis by yourself. House has a team to help him. I highly recommend using an AI agent to do the analytical heavy lifting and then gathering a group of stakeholders to review and sort through the evidence.
So, you’ve ruled a bunch of things out and zeroed in on the problem. All done. Right?
Act 3: The patient is cured?
Real life isn’t as tidy as a TV show. Most health problems aren’t caused by a single mystery disease diagnosed with simple tests. You don’t get everything wrapped up in a nice little bow by the end of the hour.4 Unfortunately, the same is true for outbound challenges. It’s rare that you’ll get a perfectly clear answer.
When presented with these kinds of ambiguities, use the differential diagnosis to identify the lowest layer of the pyramid where there’s a problem and address it. The closer it is to the foundation, the more likely it is to be—if not the direct cause—at least exacerbating the other symptoms.
Speaking of the foundation, I’ve written about the massive impact account selection has on opportunity creation. The accounts are your base. Get that part wrong and nothing above them on the pyramid will work well. When in doubt, start there.
Ultimately, you can knock out some easy wins at the top of the pyramid, but if you don’t tackle the foundational issues, it’ll be like taking medicine for a cough when it turns out you actually have leprosy.
Yes, really. And it’s kind of a real thing.
He, like me, has the gray hair to prove it.
Actually 41-44 minutes for an hour-long broadcast procedural like House. That’s a ridiculous number of commercials.
The pyramid is right, and I'd add one layer under the accounts: the data itself.
Account selection is a decision, and the decision is only as good as the company and contact data feeding it. I lived this at a previous company. Our account scoring ran on a data provider whose ratings turned out to be inaccurate. The score said "good account," reps worked the account, and they never converted to pipeline. The list looked fine. The data underneath it was wrong.
So when you say "when in doubt, start at the foundation," I'd go one step lower: audit the data before you audit the list.